
Manufactured Healthcare Deserts
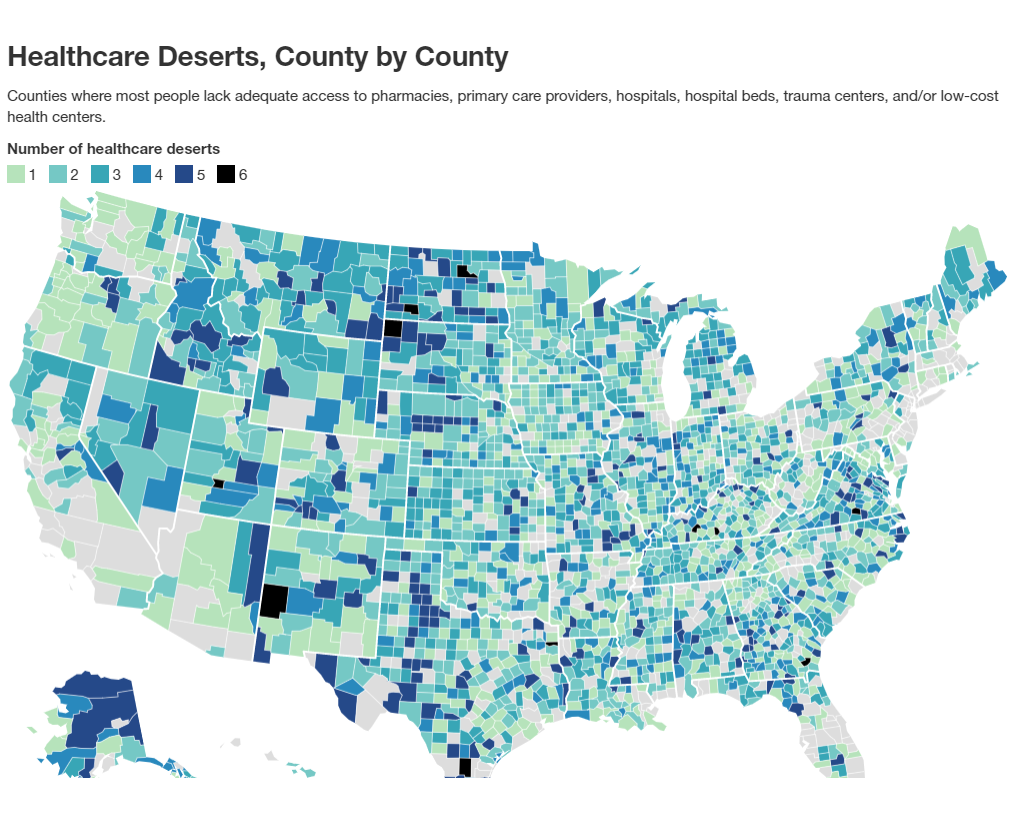
US healthcare desert data (2021)
The US spends more per capita on healthcare than any other nation, yet 35% of counties are maternity care deserts—areas with no medical facilities offering obstetric care and without a single obstetric clinician. This leaves 2.3 million people of childbearing age without access to maternity care.
Since 2018, at least 25 hospitals across Ohio have either closed or consolidated their maternity services, 10 of which served rural communities. This is only part of a broader trend occurring nationwide. Since 2022, more than 100 hospitals across the US have shut down their obstetric units. These care deserts are not accidental, nor are they specific to maternity wards; rather, they are a product of a capitalist system that prioritizes profit over the health of the working class across all medical sectors.
HEALTH & ECONOMICS
In his 1845 work The Condition of the Working Class in England, Friedrich Engels, German philosopher and co-founder of Marxism, was the first to outline the connection between poor health outcomes and the economic conditions imposed on the working class. Engels observed that the mortality rate of working-class Englishmen varied greatly from that of their bourgeois counterparts. For example, the average life expectancy for a working-class individual in Liverpool during this time was 15 years, compared to the 35 years of the upper classes.
Engels attributed this not to individual failings, but to the structural inequalities of capitalism creating environments conducive to disease and premature death. Driven by insufficient wages, the working class was, and is still, forcibly plagued by poor nutrition, housing conditions, sanitation, and other indignities, which serve as a breeding ground for contagion and epidemic.
While the specific conditions may have evolved since Engels’ time, the indignities remain. The core issues identified by Engels remain applicable to today's working class: economic inequality, labor exploitation, and inhumane working conditions. The working class continues to endure unstable employment, low wages, and long hours—all due to limited control over their labor. An excellent modern example of this is the rise of the gig economy: on-demand workers lack job security, benefits, and collective bargaining power while working jobs that pose a higher risk to their mental and physical well-being.
Engels writes, "[Society] does not trouble itself about them [workers]; leaves them to care for themselves and their families, yet supplies them no means of doing this in an efficient and permanent manner. Every working-man, even the best, is therefore constantly exposed to loss of work and food, that is to death by starvation, and many perish in this way [...] How is it possible, under such conditions, for the lower class to be healthy and long lived? What else can be expected than an excessive mortality, an unbroken series of epidemics, a progressive deterioration in the physique of the working population?"
There is no better example of this than the heightened infant and maternal mortality rates in the US. Data shows a significant portion of these deaths occur postpartum, but despite the irrefutable evidence suggesting that lack of comprehensive postpartum care is at fault, the US remains the only high-income country that does not guarantee paid maternity leave or home visits during this vital period.
The ruling class instead focuses its efforts on shifting the blame onto workers, condemning individual behaviors rather than the structural insufficiencies of capitalism. The bourgeoisie does not view public health efforts like poverty reduction and equitable access to healthcare as worthwhile investments to improve society as a whole, but rather as a means of enabling the working class's most vulnerable and disadvantaged to 'con the system'. They leave us to fight amongst ourselves for their scraps while chastising us for being hungry.
HEALTH AS A COMMODITY
Rather than a fundamental human right and public good, healthcare under capitalism is viewed as a commodity to be bought and sold. An analysis conducted by researchers at Yale School of Medicine found that, "Over the past 20 years, healthcare companies spent 95% of their net income on shareholder payouts, totaling up to $2.6 trillion.” Corporate entities are utilizing public funds to generate profit and maximize shareholder returns, yet when the working class utilizes public funds to address our basic necessities, such as SNAP benefits and Medicaid, we are vilified.
Even so-called "nonprofits" benefit from the current model under the guise of community welfare. While still taking advantage of their tax-exempt status, many nonprofit institutions expand into for-profit ventures through legal maneuvering and lax IRS oversight. The privatization of publicly funded care allows corporate entities to allocate resources to specialized services in affluent areas, while sectors like primary care and preventive services in working-class communities are neglected. The state continues to protect and appease corporate interests through patents and subsidies even as public health infrastructure erodes and essential services, such as maternity care, are abandoned en masse.
NO PROFIT NO VALUE
As private equity ownership increases, maternity services are increasingly being eliminated nationwide to redirect investments to more profitable services, such as cardiology and orthopedics. This trend is largely seen in rural and low-income areas where obstetric units often operate at a loss due to low Medicaid reimbursement rates, as they pay less than private insurers. Medicaid funding is used for four in 10 births nationwide and funds 47% of all births in rural communities.
Trump's "Big Beautiful Bill" could mean the closure of more than 140 rural labor and delivery units across the country, per National Partnership for Women & Families. These closures disproportionately impact rural and marginalized communities, leading to poorer health outcomes in a country with an already alarmingly high infant and maternal mortality rate. Quality care and community health should not be conditional on socioeconomic status or fiscal viability.
This disparity is further worsened by the overturning of Roe v. Wade, which prompted the closure of countless abortion clinics that provided essential prenatal and reproductive health services. The reallocation of funds from women's services to more 'profitable' services speaks to a broader pattern of institutionalized control over the bodies of workers. It is not enough to control your reproductive freedom; the state wants to control when, where, and how you deliver. The existing laws, economic structures, and medical practices are not for the benefit of community health and wellness, but to maintain the current social and political hierarchy.
CONCLUSION
In her 1920 work Communism and the Family, Alexandra Kollontai wrote, “Capitalism has placed a crushing burden on woman's shoulders: it has made her a wage-worker without having reduced her cares as housekeeper or mother.” This wasn’t to say women shouldn’t work, but to highlight that true equality requires not only political rights, but material support. In an ideal world, material support would be provided by the state. This would encompass maternity hospitals, childcare centers, and essential resources such as milk, food, clothing, and housing. The working class needs universally accessible maternity care centered on the well-being of parents and babies, not corporate profitability. Every parent deserves to give birth in safe conditions and with the resources they need without fear of the risk to their health and well-being.
The solutions proposed by members of the Democratic Party, such as expanding postpartum Medicaid coverage and Telehealth services, are merely reforms that, even if accomplished, can easily be taken away by the ruling class. There can be no true improvement without addressing the underlying profit motive—a deliberate structural feature of capitalism. The working class needs democratically controlled healthcare provided based on need, not ability to pay. We must fight for, and demand, a system in which healthcare is a right for all, not a commodity to be bought and sold to the highest bidder.